Archive
COVID-19 Expedient Medical Facility Options Analysis
Balancing the requirements of producing an expedient medical facility that provides sufficient overflow capacity whilst achieving the medical and engineering standards for treating COVID-19 positive patients is not an easy task. Compromise is necessary and is evident in the construction of the impressive Nightingale Hospitals that we are all familiar with, see below for a recent blog post by Jamie B.
Over the past couple of weeks I’ve conducted research into the epidemiological nature of COVID-19 and the corresponding medical and engineering requirements in order to conduct analysis and appraise alternative solutions for providing expedient medical facilities. The findings shed some light on the rationale behind the NHS Nightingale Hospitals and the potential for implementing different medical facility options.



The provision of engineering infrastructure should be dependant on the medical requirements for effectively treating COVID-19 patients whilst preventing the further transmission of the virus to health care workers.
However, there is a clear divide in medical guidance for managing COVID-19, this stems from the international community of virologists uncertainty over the causative pathogen SARS-CoV-2 and its exact mode of transmission, is it airborne? Initial research is inconclusive and the jury is still out.
This uncertainty has led to two distinct epedemiological schools of thought for managing COVID-19 patients, the cautious approach and the less cautious approach. The European Centre for Disease Prevention and Control and CDC (US counterpart) strongly endorse the provision of single patient negative pressure isolation rooms with en-suite facilities for confirmed COVID-19 cases requiring admission, where this isn’t possible cohorting of patients is recommended. Whilst the UK Government and WHO state that negative pressure isolation rooms are only required for Aerosol Generating Procedures such as intubation and cardiopulminary rescucitation due to the increased risk of airborne transmission.
Therefore there is variance in the way governments have chosen to approach the provision of COVID-19 surge capacity medical facilities, see the figures above.
My analysis of the different options has been based on the selection criteria a-f below. I conducted two iterations of a multi-criteria decision analysis (MCDA, a technique used for complex decision making) which allowed adjustment of weighting values, the first with a quality bias and the second with a cost bias (See MCDA findings below). The six distinct options chosen for evaluation were: Repurposing hospital wards, in-Situ construction of isolation units (Design similar to the USACE concept drawing), pre-fabricated cleanrooms, blu-med tented systems and the Nightingale open-patient bay design. See the one drive link below for the full study.
a. Infection Prevention and Control (IPC) Precautions. There is significant variance in the recommended IPC precautions due to the exact mode of transmission being unknown. Systems will be judged on how well they satisfy the most stringent precautions.
b. Ventilation. The system must provide ventilation in accordance with medical guidelines, designed correctly it can contain and mitigate the spread of pathogens amongst other important capabilities.
c. Power. Healthcare electrical installations must provide maximum reliability and integrity of supplies. The ideal facility will have a minimal probability of equipment failure due to loss of power.
d. Construction Time. The medical facility must have realistic construction timelines to meet surge capacity demands.
e. Cost. A key driver in all construction projects, the solution must provide benefits that are justified by the cost.
f. Surge Capacity. The solution must be capable of providing suitable patient capacity to meet surge capacity demands and have a resilient supply chain to ensure operation in the long term.
The findings recommend that in the first instance, general hospital wards should be repurposed to airborne isolation wards. The inherent advantages of locating a COVID-19 treatment facility within a hospital are obvious and there are minor cost-effective changes that can be made to increase transmission control such as adjusting existing HVAC ventilation rates for a negative pressure differential, installation of portable HEPA filtration units to improve ACH within general rooms and minor construction works such as creating ante-rooms and installing germicidal UV-C lamps at entrance points to the ward.
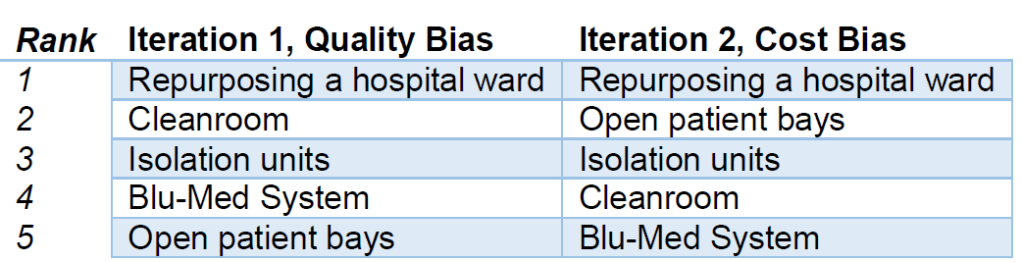
Once existing hospital space has been exhausted there are multiple options. Market research has determined cost per patient of installing a cleanroom ranges from £13,567 – 20,255 per patient with a construction time of 4 person days per patient, whereas it is estimated open patient bays can be constructed at £625 per patient at only 1.5 person days per patient. The IPC precautions and contaminant control offered by a cleanroom are superior (the ones looked at in this study conform to ISO 14644-1 Class 7 and are easily capable of 10 ACH) to the open-patient bay design and UK based companies are offering specialised COVID-19 cleanroom solutions in bulk. As alluded to in Jamie’s blog post it would be extremely difficult to provide adequate ventilation requirements in the ExCel Centre without significant modifications, personalised local ventilation would be needed for effective contaminant control.
Bespoke isolation units that can be constructed in-situ from easily available materials should not be discounted, there are proven designs described in the study that are capable of quick and cost effective construction that utilise portable HEPA units capable of 99.7% contaminant control (referred to as isolaton units in the study). These are scalable and construction materials can be swapped where applicable.
Clearly there are an inordinate amount of factors at play and the nature of the viral transmission is still unknown making decision making more complex, this blog post has only scratched the surface of the engineering challenges of each option. See the onedrive link above for more detail.
This study was completed in isolation with no involvement in the Nightingale hospital construction or COVID-19 planning teams, it is an outsiders perspective. However I hope that it provides awareness of the medical and corresponding engineering issues surrounding the best way to provide COVID-19 expedient medical facilities.
The sixth sense…
At what point in an engineers career is he able to look at a problem and sense that risks haven’t properly been addressed…?
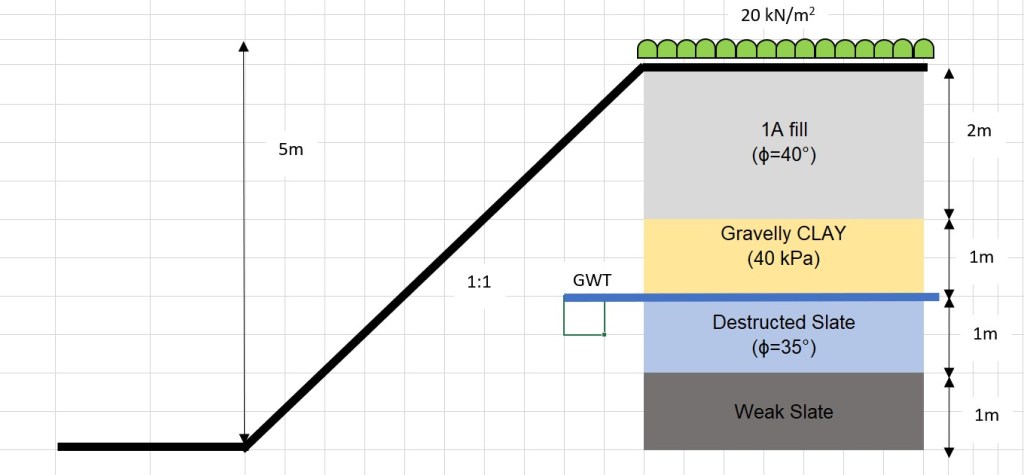
The risk in question here is safe. More specifically, slope stability of the excavation below. The slope is at a 1:1 batter at a height of 5m. The bund at the top of the slope (RHS) indicates the outer edge of the proposed site haul road (not yet operational), which will carry all laden plant. The bottom of the slope is ready for a piling mat for abutment piles. From this, I would suggest a surcharge of 20kPa at the top of the slope. The profile and design borehole is estimated below in the sketch.

Strength properties have been taken from the principal contractor’s temporary works (TW) team for other designs. If is interesting to note that most TW problems to which the site team having varying opinions
The approach/opinion to this has varied dramatically on site. The opinions are: 1) “It will be fine”, 2) “This needs assessing by TW”, 3) This is unsafe”. All project managers (10+ years experience) and all with civil engineering degrees.
What is your gut reaction? for this problem? for other problems? What problems can you rely on your heuristics to address the risks?
Experience is critical but training goes a long way.
My personal opinion (without analysis) is a suitable assessment with either GEO5 and Bishop’s method is required to propose a technical solution and manage risk. Furthermore, I would need to do some re-reading of the rock classification and discontinuities to determine if this is unsafe. I would feel semi-comfortable on doing some analysis on this and making the call on site without TW design. Perhaps a feature of a TMR in the future.
Virtual Visits So Far….
Many thanks to those I have ‘visited’ so far both for your patience and professionalism. I am looking forward to hearing from the rest of you over the coming days. From observation, MS Teams seems to be the optimum but I am waiting on WebEx for a true comparison.
COVID-19 is forcing all of us to work, think and interact in different ways and I am keen that any enduring benefits can be captured. That might be in communications, collaborative working or articulating problems and solutions. This blog offers an element of that and I would ask all of you to embrace it to improve the learning and awareness of all. Little and often is far more beneficial than war and peace every few months. A sketch or photo with a paragraph or two to generate discussion is a good starting point.
On that note we can all look forward to some posts on flooding excavations, permit to dig behaviours and others. You know who you are….
CI
Gas Holder Dumpling Slip
While we’re all sitting at home I thought I’d share this nugget from 2019 that made a little comeback in a lessons learned session we had before lock down. It is also an unexpected opportunity to use the word dumpling in an engineering context.
Back in June 2019 Keltbray were contracted to demolish two old gas holders in Sydenham. These gas holders are the large expanding “city gas” storage vessels that expand upward as gas is pumped in. The gas holders in question were of the “dumpling type” with a clay mound in the base centre of the gas holder (think the bottom of a champagne bottle). The gas holder is then partially filled with water to form an effective seal against the ground as gas is pumped in (see below).
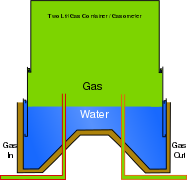
Dumpling type, two tier gas holder
As part of the dismantling sequence, the crown (lid) of the gas holder is removed, and the water and sludge is pumped out. On 12 June 2019, approximately three weeks after the pumping was completed on one of the holders, a crack through the dumpling was reported to WHP following heavy rainfall. However, the crack was first seen when the dumpling was first exposed; at the time, the crack did not alarm the site team and was considered superficial. The condition on 12 June, with the crack clearly visible, is shown below.
