Archive
Covid-19 Response; Temporary Hospital Design (Exeter)
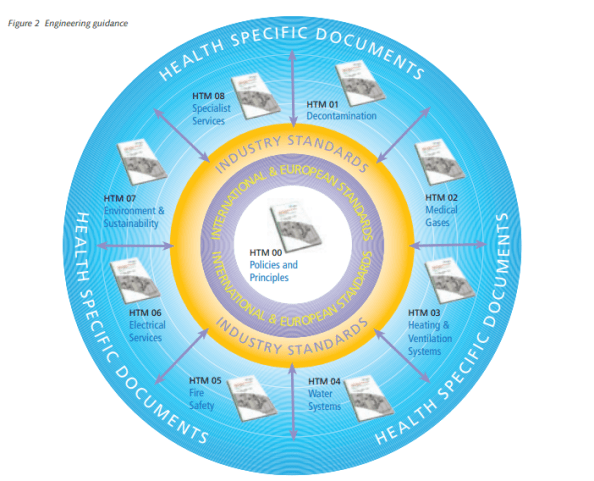
You will all be familiar with the extraordinary efforts currently going ahead to complete the 4000 bed NHS Nightingale Hospital in London. Although on a smaller scale, my design office has just been stood up en-masse to provide designs for a 500-bed facility in Exeter. Whilst waiting for the URD to be issued, we’ve all been briefed to familiarise ourselves with the requirements specified in the document:
Having reviewed the document and other relevant sources*, I wanted to give a bit of an overview of what is required from an E&M perspective, as I think the design considerations would be of particular interest in the current climate.
All Patients with suspected or confirmed COVID-19 should be placed in single rooms as shown below.

The following design requirement/ considerations are per treatment room;
Medical gases:
- Patients will need continuous medical care using piped medical gases.
- The design must be factored around the source of supply; bulk liquid oxygen plant/mini tanks/portable cylinders.
- Medical oxygen supplies must achieve a flow rate of 10 L/min, per bed (implied task; check and confirm all distribution pipe sizes).
- Distribution systems must alarm if pressure drops below 3.85 bar
- Medical air manufactured using compressors on site. It is required for driving ventilators and is supplied via a dedicated pipeline system. In addition, medical air cylinders are normally used as an independent back-up supply.
Fire:
- The use of ventilators will result in increased oxygen levels with increased risk of combustion, which should be factored into a fire risk assessment.
- Temporary fire-stopping should be provided for any wall or floor penetrations.
- Automatic smoke detection is required
HVAC:
- The density of ventilators may enrich the air with oxygen, increasing the combustion risk. To mitigate this risk the level of air changes through natural and mechanical ventilation must be maximised to lower the oxygen level to <23.5%
- Where locations are considered “early stages” or “high-risk”, patients with COVID-19 should be isolated in “negative-pressure rooms”. The recommendation is to use portable suction units which can be removed and sterilised.
Small power:
- Each treatment room requires –
- 4 x twin 13A switched sockets
- 1 x 13A cleaners socket
- Each room has a number of electronic equipment, including ventilators, for which the combined loads will need to be calculated. Diversity will be minimal as all systems will run at the same time.
Lighting:
- Each treatment room requires –
- 20-20 lux general illuminance for night-time
- 1 x 1000 lux adjustable examination lamp
- Emergency escape route lighting required: In accordance with BS 5266 and HTMs.
Domestic Hot and Coldwater:
- Each treatment room requires a hand wash basin, which should be fed through a mixer tap.
- Max hot temp = 41 dec C
- Max cold water temp , 20 dec C
- Max pipework surface temp = 43 deg C
The above detail is just taken from the one document, but the HTMs go into much more detail and will provide the basis behind any designs.
I’m sure you’ll agree there’s quite a lot to think about there… and I’m looking at 500 beds, not 4000! As a standard project, on standard timelines, all of this would not be too challenging but when considered this is all to be completed within 10 days, you can imagine the challenges with design, supply, installation and commissioning. Not to mention the unprecedented level of collaboration and coordination required.
Although the treatment room designs can be replicated for each room, the distribution and containment networks for small power, lighting, water and medical gases will require careful consideration.
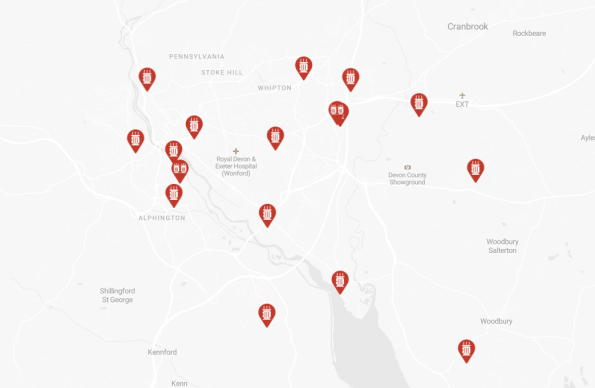
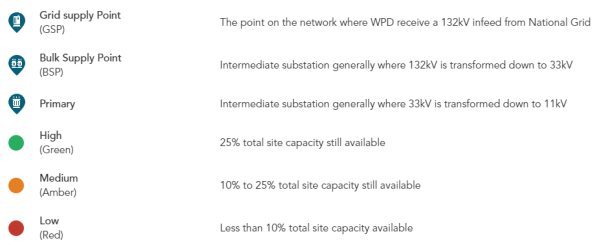
A major consideration will be the availability of supply from the local utilities companies and medical supply chains. The newly appointed site would have a much higher usage of water, electricity and gas. It will be important to calculate the requirements and engage with the utilities companies to ensure that the demand can be met. I know from recent experience that Exeter does not have a great deal of spare capacity in the electrical grid as shown below;
Hopefully, this has been of interest and given you some insight as to what is expected, with what I suspect might be the first few of many of these sites.
*A list of all relevant Health Technical Memorandums (HTMs) and Health Building Notes (HBNs) can be found on the UK Gov website HERE, but as a rough guide;